INTRODUCTION
Bartonella bacilliformis is the etiological agent of Carrion’s Disease (CD) spread by sandflies of the genus Lutzomyia. CD is endemic to Peru, Colombia, and Ecuador (1), countries whose common geographic feature is the presence of valleys and streams formed by the Andes Mountains where the temperature, humidity, and altitude are optimal for the development of ecological niches of the above vector (1). Several studies have shown that asymptomatic individuals who reside in areas of high CD endemicity serve as reservoirs for the disease because so far the infection has not been detected in animal species (2).
Given the absence of reports on CD in neighboring countries in the last few years, Peru is the only endemic country, with reports of the disease in 11 of its 24 regions, and a recent resurgence in areas of extreme poverty in Lima, Ancash, La Libertad, Piura, and Cusco, where it is currently considered endemic (3).
CD occurs as two clinical syndromes, fever leading to anemia (Oroya fever) and eruptive phase (Peruvian warts). Severity of the disease depends on the immune status of the host; some patients can develop 100% infection of erythrocytes and severe anemia with fatal consequences. In severe cases, comorbid opportunistic infections are common, which may increase morbidity and mortality rates. In endemic areas of extreme poverty, the population most affected by the chronic eruptive phase is children, who present with proliferative eruptive skin lesions and serve as the disease’s main reservoir (2,3).
Peru’s Ministry of Health
established antimicrobial therapy for CD many years ago, recommending a dose and
treatment timeline according to the clinical presentation, using chloramphenicol
(CHL) for the febrile anemic form and streptomycin or rifampicin for the
eruptive form
(4). Due to reports of therapeutic failure and persistent
bacteremia in patients treated with CHL in endemic areas, the treatment
guidelines were updated to recommend the use of second-generation quinolones,
such as ciprofloxacin (CIP), for treatment of the acute phase of CD.
Nevertheless, in recent years, there were reports of bacteriological persistence
of Bartonella bacilliformis in patients treated with CIP, after
examination of a cohort of 62 patients, 22.6% of whom had cultures positive for
the pathogen post-treatment (6).
This situation may be explained by the different mechanisms via which the
microorganism becomes CIP resistant.
Research has revealed the mechanisms of bacterial quinolone resistance: mutations or amino acid substitutions in the target sites at positions Ala91 and Asp95 of the gyrA gene, and Ala85 and Asp89 in parC; like those in Escherichia coli (Ala83 and Ala80, respectively). This is an intrinsic feature of Bartonella bacilliformis and confers constitutive resistance to nalidixic acid (first generation quinolone) due to alterations in the hydrophobicity of the targets, making the interaction of the antimicrobial agent with its target difficult (7-9). This state of affairs makes it necessary to implement a system for monitoring of the antibiotic resistance of Bartonella bacilliformis as a strategy for evaluation and control of the antibiotic sensitivity of the etiological agent of CD in order to readjust the therapeutic algorithms (1,10). On the other hand, these activities cannot be implemented in laboratories close to the endemic areas because of the special conditions this microorganism requires for its culture, isolation, and nutrition; thus, specialized laboratories are needed (10).
The laboratory protocols for identification of antibiotic sensitivity that are currently described in international guidelines consider other species of Bartonella because the cases of CD and its etiological agent, Bartonella bacilliformis, are currently being reported only in Peru. Perhaps this is why up until now there have been few studies on the antibiotic sensitivity, which also had the drawback of including very few strains; therefore, these studies do not describe the actual situation of the antibiotic resistance among strains of Bartonella bacilliformis (13,14).
Among the methods used to evaluate the antibiotic sensitivity of hard-to-grow bacteria, disk diffusion is the most common although it does not allow for analysis of Bartonella bacilliformis under usual conditions; therefore, the method needs to be adapted and other alternatives need to be devised as well (11). Taking these observations into consideration, in this study, we sought to determine in vitro resistance of strains of Bartonella bacilliformis from samples collected among patients from endemic areas of the country. We evaluated sensitivity to CHL and CIP by laboratory methods specifically designed to test antibiotic sensitivity of strains of Bartonella bacilliformis.
MATERIALS AND METHODS
A cross-sectional study was conducted, which included 100 strains of Bartonella bacilliformis from the collection of cultures of the Bartonellosis Department of the National Reference Laboratory of Metaxenic and Bacteria of the National Institute of Health of Peru, isolated from patients from endemic areas, between June 2005 and December 2011.
The selection of isolates was conducted via simple random sampling according to the availability of strains in an endemic area and included strains obtained from CD outbreaks: 30 from Huarochirí-Lima (2005), 20 from Jaén and ChotaCajamarca (2007), 30 from Quillabamba-Cusco (2008-2009), 15 from Caraz-Ancash (2011), and 5 from PatazLa Libertad (2011). All isolates available from Ancash, Cajamarca, and La Libertad were also evaluated (40 strains).
The in vitro assay of antibiotic sensitivity of Bartonella bacilliformis to CHL and CIP was developed from three microbiological methods: disk diffusion, E-test, and agar dilution, which were specifically adapted to this microorganism. The following reference strains were used as controls: Bartonella bacilliformis ATCC35685 and Escherichia coli 25922.
STRAIN REACTIVATION
Cryopreserved strains of Bartonella bacilliformis were removed from the freezer at −80ºC and were inoculated into a two-phase medium with solid-phase Columbia agar (Oxoid), 0.25% yeast extract (Difco), 10% defibrinated sheep blood, and RPMI 1640 (Gibco) with L-glutamine and liquid-phase sodium bicarbonate. The inoculated flasks were incubated at 28–30ºC for 4 to 5 days, after which they were subcultured in Columbia blood agar plates and inoculated (0.5 mL) into the liquid phase based on positive cultures. The plates were incubated at 28–30°C for 3 to 4 days until we observed confluent growth of the microorganism colonies.
SENSITIVITY EVALUATION
Preparation of sensitivity
assay plates for disk diffusion and E-test methods. For in vitro
evaluation of the sensitivity of Bartonella bacilliformis to CHL and CIP,
we modified and adapted the procedures of the sensitivity assays, incubation
periods, and culture medium to be used. For the disk diffusion and E-test
methods, we prepared Columbia agar plates supplemented with 10% defibrinated
sheep blood. The volume of agar dispensed per plate was 35 mL, with an average
height of 4 mm as recommended by the Clinical and Laboratory Standards Institute
(CLSI).
Preparation of plates with antibiotic dilutions. We prepared two dilutions of the antibiotics (active drug) CHL and CIP (Sigma) in decreasing order: 128 to 0.0312 µg/mL. Each antibiotic dilution was homogenized in the Columbia blood agar medium with 10% sheep blood and poured into sterile plates.
Inoculum standardization for disk diffusion and E-test methods. We standardized the bacterial inoculum of Bartonella bacilliformis using a subculture plate with confluent growth of the microorganism colonies, which were resuspended in 5 mL of sterile physiological saline, conforming to the turbidity standard of 0.5 on McFarland’s scale, which corresponds to 1.5 × 108 CFU/mL; this parameter was immediately verified with a turbidimeter.
Inoculation of plates for sensitivity testing. We distributed 0.5 mL of the standardized bacterial inoculum homogeneously across the surface of the blood agar in order to achieve confluent growth of the microorganism. Once the inoculum was incorporated into the medium, sensitivity disks and E-test strips for both antimicrobial agents were added. The plates were incubated at 28ºC to 30ºC for 6 days.
Inoculation of plates with antibiotic dilutions. the bacterial inocula of each strain were normalized to 0.5 on McFarland’s scale; each inoculum was diluted to 1/100, and finally 400 µL of each dilution was placed individually in the wells of a Steers replicator. Using the Steers inoculator, we dispensed 10 µL of the bacterial inoculum on the surface of the agar plates that contained increasing concentrations of the antimicrobials. The plates were incubated at 28–30ºC for 6 days.
Analysis of the disk diffusion plates.The plates were examined under indirect light, and each halo of inhibition around the antibiotic disks was measured: CIP 5 µg and CHL 30 µg (®Oxoid). The cases that showed growth up to the edge of the disk were labeled with the value of the disk diameter (6 mm). Once the values were obtained, the strains were designated as either sensitive or resistant.
Analysis of E-test plates. We used strips of CHL (0.016–256 µg/mL range) and CIP (0.002–32 µg/mL; BioMerieux). We determined the minimum inhibitory concentration (MIC) of each antibiotic by examining the interface of the ellipse formed between bacterial growth and the inhibition thereof.
Analysis of agar dilution plates.After 6 days of incubation, the inoculated plates were examined under direct light. We observed growth at the inoculation points, determined the MIC, and identified the antibiotic dilutions that completely inhibited the bacterial growth.
Determination of cut-off points and inhibition zones for the antibiotic sensitivity assay of Bartonella bacilliformis. Given the absence of cut-off points established by the CLSI or any other international institutions for Bartonella bacilliformis, the National Reference Laboratory of Metaxenic and Bacteria of the National Institute of Health of Peru, in accordance with the methodology established by the British Society for Antimicrobial Chemotherapy (BSAC), determined the cut-off points of both antimicrobial agents for the E-test and agar dilution methods, taking into account the pharmacokinetic information: CIP (sensitive: ≤0.5 µg/mL, resistant: ≥1 µg/mL) and CHL (sensitive: ≤0.5 µg/mL, resistant: ≥1 µg/mL) and for the disk diffusion method (sensitive: ≥21 mm and resistant: ≤20 mm).
DATA ANALYSIS
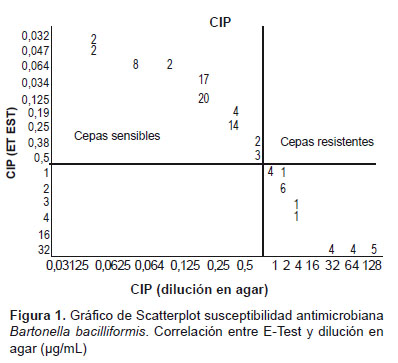
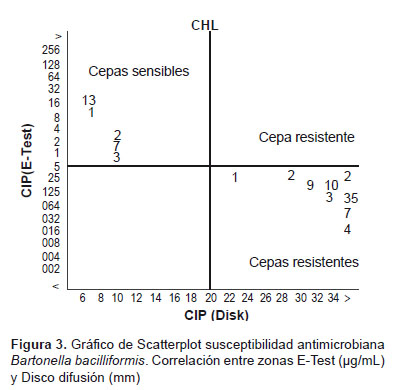
Next, analysis of the results on the antibiotic sensitivity of each isolate was entered into the STATA software v. 12.0 to calculate the statistically valid cut-off points for both antimicrobial agents. In order to determine the correlation between the MIC (µg/mL) and the diameter of the inhibition zone in the disk diffusion test for each antimicrobial agent, we used the WHONET software and its scatter plot graphs(19,20).
The frequencies of CHL- and CIP-sensitive and -resistant strains of Bartonella bacilliformis were determined by three laboratory methods. These frequencies were calculated in percentages corresponding to the endemicareas. To evaluate the association between resistant strains and the patients’ prior antimicrobial treatment, we used the tetrachoric correlation coefficient and STATA software v. 12.0.
ETHICAL CONSIDERATIONS
Each evaluated strain was coded in order to maintain confidentiality of the information. The study protocol was approved by the Research and Ethics Committee of the National Institute of Health of Peru.
RESULTS
The cut-off points for the evaluation of antibiotic sensitivity of the strains of Bartonella bacilliformis toward CHL and CIP, using the E-test, agar dilution, or disk diffusion methods, using Columbia agar supplemented with 10% defibrinated sheep blood, were established for the microorganism in this study, in accordance with the methodology of the BSAC.
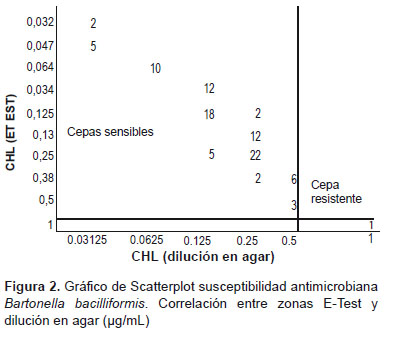
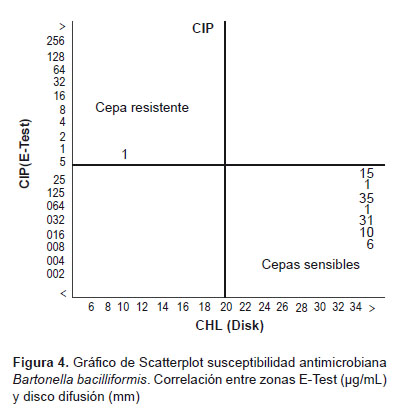
The statistically determined cut-off points were identical for CHP and CIP, after we obtained the following values for the agar dilution and E-test methods: ≤0.5 µg/mL (sensitive strains) and ≥1 µg/mL (resistant strains). For disk diffusion, the values obtained from the diameter of the inhibition halos for both antimicrobial agents were ≥21 mm (sensitive strains) and ≤20 mm (resistant strains). The resulting scatter plot allows for direct comparison of the isolate results according to the evaluated methods. This analysis confirmed a positive correlation between the MIC values and the inhibition zones in the three evaluated methods, after we obtained the same results for both sensitive and resistant strains (Figures 1–4).
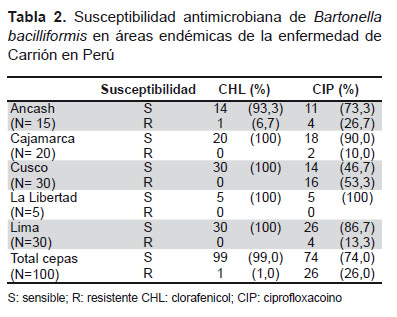
Using the cut-off points established during our research, the in vitro phenotypic resistance to CIP among the 100 strains that we evaluated was 26%, and only 1% of the strains were resistant to CHL. The greatest number of CIP-resistant strains came from Quillabamba-Cusco (16/26; 61.5%), Huarochirí-Lima (4/26; 15.4%), Ancash, (4/26; 15.4%), and Jaén-Cajamarca (2/26; 7.7%). The CHL-resistant strain was isolated from a patient in Ancash (1/100; 1%; Table 3). It was not possible to conduct a precise comparison of the in vitro phenotypic resistance of all the Bartonella bacilliformis strains circulating in every endemic region of Peru because of the limited availability of isolates, especially in La Libertad.
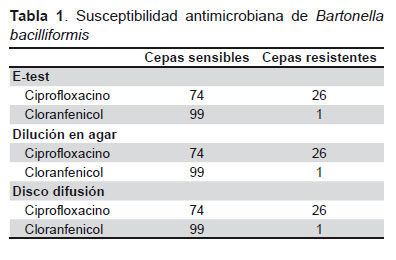
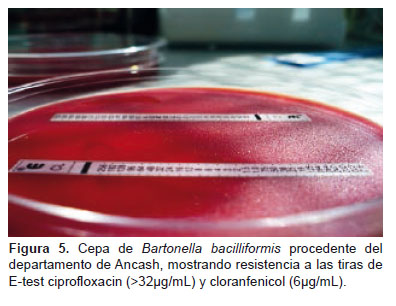
During evaluation of the antibiotic sensitivity by the E-test method, 74 strains showed inhibition of bacterial growth at MICs of CIP 0.016–0.5 µg/mL, thus confirming their sensitivity to the antibiotic. The same was observed among 99 isolates exposed to CHL strips; 26 strains showed different patterns, 13 isolates grew at the maximum CIP concentration (>32 µg/mL; Figure 3), and the remaining 13 strains grew at the concentrations ≥1–4 µg/mL, thereby proving to be resistant to this antimicrobial agent in vitro. One strain showed growth up to the concentration 6 µg/mL in the CHL strip (Figures 1 and 2).
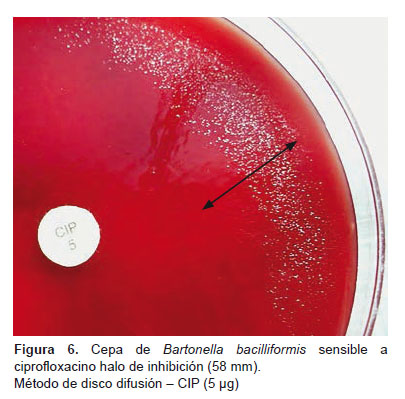
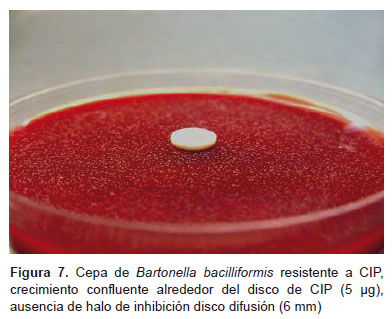
The 74 strains that were identified as sensitive by the E-test method showed inhibition halos between 40 and 58 mm around the CIP disks (5 µg) and CHL disks (30 µg), thus confirming their sensitivity to both antibiotics according to the disk diffusion method (Figure 5). With this method, the 26 strains identified as resistant by the E-test shared similar inhibition patterns with the CIP disks; 14 isolates showed confluent growth of colonies around the disk (Figure 7); 8 strains yielded inhibition halos between 17 and 18 mm, and the remaining 4 had halos between 19 and 20 mm. As for CHL, one strain had a halo of 17 mm.
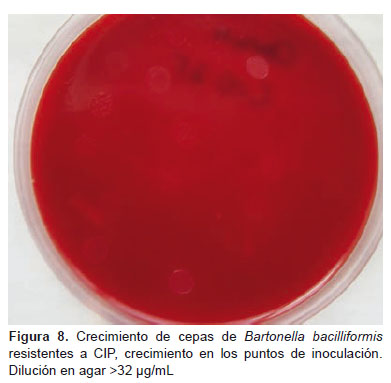
The agar dilution method confirmed the results obtained with the other methods that we evaluated; 74 strains grew in plates at CIP concentrations between 0.0312 and 0.5 µg/mL, 26 strains showed growth at the inoculation sites in plates with concentrations >1 µg/mL; 13 isolates grew in plates with concentrations >32 µg/mL. Regarding CHL, there was bacterial growth of 99 strains in plates with antibiotic concentrations between 0.0312 and 0.5 µg/mL. Only one strain grew at concentrations of up to 16 µg/mL (Figures 1 and 2).
It was determined via review of the medical histories of the patients (from whom the 26 CIP-resistant strains came) that 17 of them never received CIP treatment while the remaining 9 patients received CIP at 500 mg per 12 hours for 10 days. The patient from whom the CHL-resistant strain came never received any antibiotic treatment.
During the statistical evaluation of these results, by means of the STATA v. 12.0 tetrachoric correlation coefficient, we obtained a value of p < 0.0001 for both cases, demonstrating that there was no relation between antibiotic resistance and the treatment received.
DISCUSSION
National and international studies on antibiotic sensitivity of Bartonella bacilliformis strains in vitro by means of the plate microdilution method and/or E-test method determined that Bartonella bacilliformis and other species of this genus are highly sensitive to most of antimicrobial drugs such as β-lactams, penicillin, aminoglycosides, cephalosporins, and quinolones (12,14). In contrast, our study shows elevated resistance to CIP and almost no resistance to CHL; this finding was unexpected given that this medication is no longer used due to frequent reports of a lack of a clinical response. These results are probably due to the small number of strains evaluated from the region of Ancash, where failures of CHL therapy were reported. Regarding CIP resistance, this medication is considered first-line treatment of CD in different guidelines, both national and international (4,5,6,15); this position should be reevaluated.
The differences with other studies may be due to the fact that these studies were conducted on only a small number of Bartonella bacilliformis (13) strains; therefore, the results may not be significant and may not reflect either the real situation (in terms of the in vitro antibiotic sensitivity of Bartonella bacilliformis strains) or the actual prevalence of probably resistant strains circulating in Peru. Furthermore, indiscriminate use of CIP and other antibiotics may have affected the results of these studies (9). This situation can explain the current cases where the antibiotic therapy established for the treatment of patients with CD has failed.
Bartonella bacilliformis is a slow-growing organism that requires an enriched medium and optimal temperature for its growth. This is why the three laboratory methods that we implemented were specifically designed and adapted to this study. We found that the E-test method and disk diffusion method are the most convenient for evaluation of the in vitro antibiotic sensitivity of Bartonella bacilliformis strains. This is because these methods can be easily implemented in medium-size laboratories, whereas the agar dilution method has the disadvantages of the high cost of the reagents as well as the laborious procedures for its implementation.
In this study, we evaluated in vitro antibiotic sensitivity of 100 strains of Bartonella bacilliformis from five endemic areas with frequent outbreaks of the disease. The highest percentage (16%) of CIP-resistant strains came from the region of Cusco, where one of the latest important outbreaks was recorded in 2002 after El Niño (16), and subsequently in 2008 and 2009. The strains that we studied here were isolated during these periods (2008 and 2009). The limited number of strains available in the regions of La Libertad and Ancash made it impossible to obtain representative information on the actual situation regarding the in vitro antibiotic sensitivity of Bartonella bacilliformis strains circulating in the two regions, especially in Ancash, where frequent failures of CHL were reported for the patients treated with this antibiotic.
It is worth mentioning that there are no strains available from the big outbreaks of 2002–2004 in Cusco and Ancash, which is why it was not possible to include this important group in our study.
CIP resistance is not new; other studies (that have utilized various molecular procedures to evaluate strains of Bartonella bacilliformis isolated in 1957, 1970, and 1996) revealed that these strains have constitutive quinolone resistance related to the presence of alanine in positions 91 and 85 of the quinolone targets (GyrA and ParC) (7,8). These results were already alerting us to their intrinsic and constitutive resistance before the introduction of quinolones into clinical practice. This is why their inclusion in the technical regulations (as well as in clinical recommendations regarding the use of CIP for the treatment of CD in Peru) should be reevaluated, given the rapidly developing resistance among these strains.
This is important in the Peruvian context, because evaluation of the effectiveness of antimicrobial treatment of CD is currently performed only in clinical settings, depending on the clinical course and therapeutic response of a patient. To date, no studies have been conducted regarding bacteriological evaluation of antibiotics after treatment has been completed. These studies, if performed, should provide crucial evidence of the in vitro behavior of the microorganism in response to the antimicrobial therapy used. If the main reservoir is the person who had the disease, then the best antibiotic would be the one that eliminates the bacteremia after treatment, thus becoming the main measure of CD prevention and control in endemic areas. These recommendations are for future research.
Our study has some limitations; the number of strains is not representative of the whole Peru although our set of isolates corresponds to approximately 50% of the strains isolated in the 2005–2011 period by the Laboratory of Metaxenic and Bacteria of the National Institute of Health. The latter is the reference center in Peru for bacteriological characterization of Bartonella bacilliformis. Currently, we are evaluating sensitivity to aminoglycosides, to other fluoroquinolones, to macrolides, penicillins, cephalosporins, tetracycline, and others. We are also characterizing the genes involved in the genotypic resistance to antibiotics in this microorganism. The study in progress is expected to complement the results obtained so far.
In conclusion, this paper seems to be the first report that includes a number of important Bartonella bacilliformis strains that show elevated levels of in vitro antibiotic resistance: in 26% of Bartonella bacilliformis strains to second-generation quinolones (CIP), unlike the 1% resistance to CHL that we observed here. Using the three methods, we obtained similar results for each strain that was studied; thus, our results confirm the in vitro sensitivity or resistance of a Bartonella bacilliformis strain to CIP and CHL.
Therefore, we propose reevaluating the therapeutic regimens currently used for antimicrobial therapy of patients with CD. Likewise, it is necessary to strengthen the system for monitoring of the antibiotic resistance of Bartonella bacilliformisstrains on the national level, and to continue research into the molecular mechanisms by which this microorganism evades the action of the antibiotics that have been used to date.
Acknowledgments:We would like to thank Dr. Charles Huamaní for the advice regarding the writing of this manuscript.
Author Contributions: GMM participated in the conception and design of the study, analysis, data interpretation, and drafting of the manuscript. DFL participated in the analysis, data interpretation, and drafting of the manuscript. All coauthors critically reviewed the preliminary drafts of the manuscript and approved the final draft.
Funding Source: National Institute of Health of Peru.
Conflicts of Interest: The authors declare that they have no approved the final draft. conflicts of interest related to publication of this article.
References
1. Nunura JM. La Vigilancia Epidemiológica en Salud Pública de la enfermedad de Carrión. Bol Epidemiol (Lima). 2012;21(15):245-46.
2. Bass JW, Vincent JM, Person DA. The expanding espectrum of Bartonella infections: I. Bartonellosis and trench fever . Pediatr Infect Dis J. 1997;16(1):2-10.
3. Ministerios de Salud del Perú. Enfermedad de Carrión (bartonelosis) en el Perú. Módulos Técnicos. Serie de documentos monográficos. Lima: MINSA/INS; 2001.
4. Tarazona A, Maguiña C, López de Guimaraes D, Montoya M, Pachas P. Terapia antibiótica para el manejo de la Bartonelosis o enfermedad de Carrión en el Perú . Rev Peru Med Exp Salud Publica. 2006;23(3):188-200.
5. Norma Técnica para la Atención de la Bartonelosis o Enfermedad de Carrión en el Perú. NTS Nº 048-MINSA/DGSP-V.01; Lima. (Julio del 2006).
6. Pachas P. Generando evidencias para las políticas públicas de prevención y control: Experiencia en la enfermedad de Carrión en el Perú [internet]. En: VII Congreso Científico Internacional del Instituto Nacional de Salud, Lima, Perú. 07 al 09 de noviembre de 2013 [citado el 14 de julio de 2015]. Disponible en: http://www.bvs.ins.gob.pe/congresos/index.php/2013-11-05-19-25-01/congreso#jueves-7-mañana
7. del Valle LJ, Flores L, Vargas M, Garcia-de-la-Guarda R, Quispe RL, Ibañez ZB, et al. Bartonella bacilliformis, endemic pathogen of the Andean region, is intrinsically resistant to quinolones . Int J Infect Dis. 2010;14(6):506-10. doi: 10.1016/j.ijid.2009.07.025.
8. Minnick MF, Wilson ZR, Smitherman LS, Samuels DS. gyrA mutations in ciprofloxacin-resistant Bartonella bacilliformis strains obtained in vitro . Antimicrob Agents Chemother. 2011;47(1):383-6.
9. Biswas S, Raoult D, Rolain JM. Molecular mechanisms of resistance to antibiotics in Bartonella bacilliformis . J Antimicrob Chemother. 2007;59(6):1065-70.
10. Sánchez Clemente N, Ugarte-Gil CA, Solórzano N, Maguiña C, Pachas P, Blazes D, et al. Bartonella bacilliformis: a systematic review of the literature to guide the research agenda for elimination . PLoS Negl Trop Dis. 2012;6(10):e1819. doi: 10.1371/journal.pntd.0001819.
11. Ives TJ, Manzewitsch P, Regnery RL, Butts JD, Kebede M. In vitro susceptibilities of Bartonella henselae, B. quintana, B. elizabethae, Rickettsia rickettsii, R. conorii, R. akari, and R. prowazekii to macrolide antibiotics as determined by immunofluorescent-antibody analysis of infected Vero cell monolayers . Antimicrob Agents Chemother. 1997;41(3):578-82.
12. Dörbecker C, Sander A, Oberle K, Schulin-Casonato T. In vitro susceptibility of Bartonella species to 17 antimicrobial compounds: comparison of Etest and agar dilution . J Antimicrob Chemother. 2006;58(4):784-8.
13. Sobraqués M, Maurin M, Birtles RJ, Raoult D. In vitro susceptibilities of four Bartonella bacilliformis strains to 30 antibiotic compounds . Antimicrob Agents Chemother. 1999;43(8):2090-2.
14. Novelli S. Determinación de la susceptibilidad antibiótica de 14 antibióticos para Bartonella bacilliformis por métodos microbiológicos e inmunohistoquímicos [Tesis bachiller]. Lima: Universidad Peruana Cayetano Hredia; 2004.
15. Pérez-Martínez L, Blanco JR, Oteo JA. [Treatment of human infections caused by Bartonella spp.] . Rev Esp Quimioter. 2010;23(3):109-14. [Article in Spanish]
16. Quispe R. Caracterización molecular de los genes asociados a la resistencia antimicrobiana en Bartonella bacilliformis [Tesis bachiller]. Lima: Facultad de Ciencias Biológicas, UNMSM; 2009.
17. Ruiz J. Mechanisms of resistance to quinolones: target alterations, decreased accumulation and DNA gyrase protection . J Antimicrob Chemother. 2003;51(5):1109-17.
18. Tarazona D, Padilla C, Caceres O, Montenegro JD, Bailon H, Ventura G, et al. Whole Genome Sequencing and Comparative Analysis of Bartonella bacilliformis Strain INS, the Causative Agent of Carrion’s Disease . Genome Announc. 2013;1(1). pii: e00053-12. doi: 10.1128/genomeA.00053-12.
19. Mac Gowan AP, Wise R. Establishing MIC breakpoints and the interpretation of in vitro susceptibility tests . J Antimicrob Chemother. 2001;48 Suppl 1:17-28.
20. British Medical Association and Royal Pharmaceutical Society of Great Britain. British National Formulary, 40th ed. London: British Medical Association and Royal Pharmaceutical Society of Great Britain, 2000.
Correspondence: Giovanna Mendoza Mujica
Address:
Capac Yupanqui 1400 Jesus Maria, Lima 11, Peru
Phone number:
(511) 7481111 Ext. 2134
E-mail:
gmendoza@ins.gob.pe, gmm2407@ gmail.com
Received: 8/13/2015
Approved: 10/21/2015