Andrés A. Agudelo-Suárez
Diego A. Restrepo-Ochoa
ORIGINAL ARTICLE
Relations established by women during pregnancy,
delivery and postpartum with health personnel according to social class in
Bogotá: qualitative study
Libia
A. Bedoya-Ruiz ![]() 1,
Physician, Master in Public
Health
1,
Physician, Master in Public
Health
Andrés
A. Agudelo-Suárez ![]() 1,2, odontologist, doctor of Public
Health
1,2, odontologist, doctor of Public
Health
Diego
A. Restrepo-Ochoa ![]() 1,3, psychologist, doctor of Public
Health
1,3, psychologist, doctor of Public
Health
1 Escuela de Graduados, Universidad CES,
Medellin, Colombia.
2 Facultad de Odontología, Universidad de
Antioquia, Medellin, Colombia.
3 Facultad de Psicología, Universidad CES,
Medellin, Colombia.
This research is an academic product from: Bedoya Ruiz LA. Composition of the relationship of women in pregnancy, labor and postpartum with healthcare services at different levels according to social class. Bogotá, Colombia. [Doctoral thesis]. Medellín: Escuela de Graduados, Universidad CES de Medellín; 2020.
ABSTRACT
Objective: To understand the relationship
established between women in a situation of pregnancy, childbirth and
postpartum with the health services personnel according to social class in
Bogotá (Colombia).
Materials and methods: Qualitative study. Critical
hermeneutical perspective and critical ethnography. Theoretical sampling.
Analysis by triangulation in Atlas.ti. 9 women and 8 health professionals
participated. 38 in-depth interviews were conducted for 13 months and 62
accompaniments to the maternal in the activities of prenatal control,
vaccination, labor, postpartum consultation, follow-up exams, prophylactic pisco
course, hospitalization and waiting room, both in public services as private.
Results: There are inequalities according to social class in which the
relationship between women and staff is configured in the following aspects:
permeability to the needs of women, recognition of psychosocial aspects, having
different points of view against a medical recommendation and right to complain
or demand to improve.
Conclusions: The situation described above intensifies gender issues in women with a less advantageous social class. It is necessary to develop interventions in educational and health institutions that consider aspects where human resources are sensitized on social issues related to the theoretical proposals of research and the democratization of medical information. It is unfair that the condition of social class and gender affects the quality of care and economically stratifies people’s rights.
Keywords: Social Class; Interpersonal
Relations; Pregnancy; Childbirth; Postpartum Period (source:
INTRODUCTION
There is evidence from all over the world demonstrating
mistreatment of women during pregnancy, labor and postpartum (PLP) by
healthcare personnel (1,2). Even when public healthcare programs were introduced
to implement respectful maternity care, the effects of these interventions were
not satisfactory in all cases —physical abuse decreased, but other situations
such as verbal abuse, neglect, and abandonment (1) did not.
The relationship between healthcare personnel and
women during PLP is also a concern in Colombia, where investigations carried
out revealed obstetric and gender violence (3-8). Previous studies, which
were carried out with women of different educational levels, failed to evidence
the inequalities in relationships depending on social classes. This shows
conceptual and methodological gaps in public healthcare research on this topic (9),
making it necessary not only to deepen into the indicators of maternal
morbidity and mortality, but also to the quality of health care.
|
KEY MESSAGES
|
|
Motivation for the study:
It is important to evidence the gaps in the literature, taking
into account that women in pregnancy, labor and postpartum are frequently
overlooked as subjects by health professionals.
Main findings:
There
are inequalities in the relationship that women establish with healthcare
personnel according to social class.
Implications: Alternatives must be found in the care process that transcend
the traditional biomedical model. Health policies require important
transformations in the medical and health education system. |
This study is specifically based on theories proposed by Breilh
and Menéndez (10-13). On the one hand, Breilh’s position is neo-Marxist,
that is to say, social class is not a personal choice but determined by
structural aspects. Thus, health inequalities reflect social inequalities. In
this sense, social class is understood as a group of people who share common
interests but have different levels of power, depending on their hierarchies in
the work process, and this determines their ability to accumulate wealth (10,11).
On the other hand, Menéndez focuses on critical
medical anthropology, based not only on cultural differences (seen as a barrier
between the biomedical system and the popular medical system), since it is also
necessary to include aspects related to poverty and social inequalities (12,13).
The concept of a hegemonic medical model not only ideologically excludes the
knowledge historically constructed by the subjects, but also ignores the
poorest people and ethnic groups (12,13).
On the basis of the above said, the objective of this study was to understand the relationship established between women during PLP with healthcare service depending on social class in the city of Bogota (Colombia).
MATERIALS AND
METHODS
Qualitative
and flexible study (18,19) carried out with a theoretical and methodological
approach, modified according to findings during the fieldwork. It was detailed
in a methodological report (19) and reviewed by the research committee and
external evaluators (reliability and auditability).
Phases of the
study and participants
The exploration began in May 2017, and the fieldwork began in
November 2017 and ended in December 2018. This phase consisted on personal
interviews as well as virtual communications through social networks, which
created an environment of trust among the participants —the subjects could
freely express their thoughts whenever they wanted. The analysis and writing of
the information began during the fieldwork and ended in November 2019.
During this phase of the study, nine women from the
city of Bogota, at least in the first trimester of pregnancy, and eight
healthcare professionals whose sociodemographic characteristics are summarized
in Tables 1 and 2. Women with mental illnesses or disabilities, minors and
those who could change their residence did not participate. Women and
healthcare personnel were contacted through social networks and the public
sector prenatal monitoring service, three women refused to participate because
they did not need the proposed support.
Table 1.
Sociodemographic
characteristics of pregnant women participating in the research. Bogota

a Socioeconomic status. There are 6 status considered in Colombia, with 1 being the lowest and 6 the highest. This stratification is made according to the place of housing.
b Although two women have
complementary plans, the companies that provide the healthcare services are
different and therefore the clinics are different. This is also the case in the
contributory and subsidized regime. Therefore, the first letter is placed to
make visible the companies that are different. c
Families that have the capacity to sabe and receive income from sources other
than work (rentals, equipment rental). d
Subsidized EPS. e Financial fund. f Vulnerable localities in the south of Bogotá
with worse maternal and fetal health indicators, environmental contamination,
deficit of public transport, insecurity, deficit of health services, prolonged
transfers between home and
Table 2.
Characteristics
of healthcare personnel with experience in maternal care participating in the
study, Bogota.
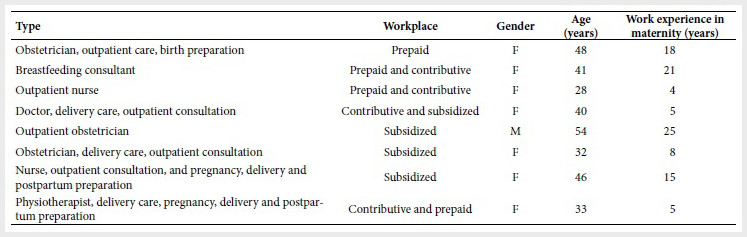
F: Female; M: Male
Procedure
Epistemological perspective
This
perspective considered critical hermeneutics, i. e., elements from hermeneutics
and elements from critical theory. Gadamer explains that the interpretation of
hermeneutics is not “a reproduction of an original production” but a
researcher-researched mediation, therefore it requires understanding, which is
far from objectivity. Preconceptions are built by life experiences; this
concept determines the way in which a subject can be interpreted (14).
Habbermas combines interpretation and critical theory that requires objectivity
to analyze the material conditions of the population. This author argues that
preconceptions are not always legitimate, because traditions can be imposed,
interpretation should serve to criticize ideology. Even if necessary, for understanding
the subject’s point of view, interpretation also reveals power relationships
that allow developing emancipation (15). The foregoing accounts for
the complexity of epistemology —bricoleur researchers do not limit themselves
to produce meanings of pure hermeneutics, since they can generate a resistance
to the transformation of social conditions (16).
Method
Critical
ethnography from Menendez’s relational approach that links micro-social
(relationship between subjects) and macro-social aspects (structural
conditions) (13),
and Sheper-Hughes’ position regarding the role of the researcher, who does not
try to blend in with the population, but rather realizes that his or her
presence in the community will transform his or her life and that of the
subjects of study, for this reason, it questions in a respectful and critical
manner, the health situations normalized by the population, which are aspects
that contribute to oppression in the midst of poverty and inequality. However,
this dialogue is bilateral, since it also allows the population to question it
and things are learned from this as well (17).
Quality criteria
Credibility and reliability were evaluated (13,18,19),
taking into account the participation of the main researcher who could change
the subjects’ behavior. During the fieldwork, situations affecting women’s
sexual and reproductive rights were revealed. In some cases, the participants
normalized this situation and did not see the problem; in other cases, they
sought help from the researcher. The principal investigator provided documented
information related to rights, helped to clarify medical terms, asked questions
about their wishes and opportunities, and contacted support networks on sexual
and reproductive healthcare and state institutions that monitor health care
services. It all was done for women to have tools when making their own
decisions so themselves, not the researcher, could be the transformers of the
situations that occurred in the healthcare services, all of which is consistent
with the epistemological paradigm chosen. The reference framework was built
throughout the research process, which allowed, at the end of the research, the
analysis of the results from different theoretical perspectives (credibility).
In the writing process, the discourses of the
actors were differentiated from the analyses carried out by the researcher. The
information recorded was made available to external evaluators who so they can
verify the results found (reliability and auditability).
Sampling
Theoretical
sampling (19),
taking into account Breilh’s concepts of social class (10,11) and the type of health affiliation in Colombia
(20).
Three categories were differentiated according to the work situation related to
social class (21): subsidized regime (women with informal work,
population without payment capacity), basic contributory regime (salaried
women), and prepaid contributory regime or plans complementary (salaried women
or businesswomen with the ability to pay for private services).
Methodological strategies and techniques
Three to five in-depth interviews were conducted per woman
during the PLP (with a live newborn) and information was collected at different
points in the research process (credibility). Counting the healthcare
personnel, there were a total of 38 interviews.
The interviews were carried out by the main
researcher in an unstructured way with open questions (22). A
guide was used that included topics related to social class (9-11) and the meanings of the relationship of women
with healthcare personnel (9,12). The meetings were scheduled
according to the availability of the participants in places chosen by them. The
conversations were private and confidential: in social organizations, the home
when the women were alone, and little frequented restaurants. The duration was
one hour on average.
The main researcher carried out the participant
observation (13,23) in the health services where the women
attended (Table 1). 62 women were accompanied during pregnancy, labor and
postpartum. The observations were recorded in a field diary. We sought not to
block interaction with subjects. The complete writing was done when not in the
field. Accompaniment itineraries were constructed in an ethnographic manner,
with descriptive and detailed information (credibility) that included: point of
view of each woman (visibility of the PLP process in a historical and situated
context), the position of other subjects different from the participants
(credibility), the established dialogues and the reflexivity of the researcher.
Statistical and epidemiological information was collected and it was used to
build the context of the research, which helped to give meaning to the results.
All of the above is available at Escuela de Graduados of Universidad CES in
Medellin to inform of the transferability to other Latin American urban
contexts with similar health systems.
Qualitative
analysis
Similar and different aspects among participants were identified
in the accompaniment itineraries. This information was organized during the
PLP, which allowed us to see recurrence of theoretical aspects over time by
each woman (23).
The above was transcribed in an Excel file which was important to analyze the
interviews, since there were aspects that seemed to be non-recurring, but when
triangulated (credibility) with the accompaniment itineraries, they acquired
theoretical importance.
The interviews were recorded by the main researcher
and transcribed by two female transcribers from Universidad CES in Medellin.
The transcriptions of the interviews and the accompaniment itinerary were given
to the participants for feedback.
ATLAS.ti 7 was used for the analysis; a code was
assigned to the paragraphs or phrases, which allowed classifying the information.
We disaggregated data so we could link them again but in a different way, in
the form of categories. This was done seeking to construct concepts related to
the theory (content analysis) and group data that have similar meanings, in
order to construct concepts that give meaning to the results (24). We
could identify 179 codes derived from the data and organized them in 11
categories. Two categories are published in the results of this article. The
coding process was carried out with the research group and a social worker.
The results were triangulated taking into account
the methodological techniques (credibility) and the socialization process (18,19).
This was carried out with peer researchers from Universidad CES and experts in
the field, outside the process, which allowed the inclusion of different and
interdisciplinary perspectives (reliability, auditability). Likewise, the
socialization was progressive with the participants to validate the information
and propose strategies that emerge from themselves.
Ethical aspects
We
obtained the approval of Universidad CES Ethics Committee (Act No. 99/2016) and
the Secretary of Health of Bogota (Act No. N0041000/2017). According to the
Colombian Code of Medical Ethics, the clinical decisions made by healthcare
personnel were respected in the medical field, since the attention given by
healthcare workers excluded the possible medical attention required from the
principal investigator. In the informed consent, it was clarified who the
researcher was and her interests as a woman, a physician and a mother.
RESULTS
The
following two categories were found (Figure 1).
PLP: pregnancy, labor and postpartum
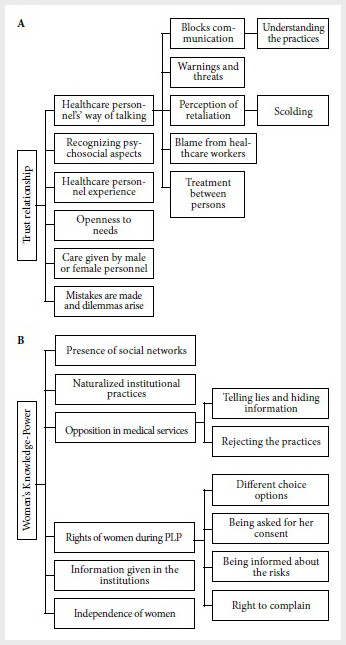
Figure 1. A. Trust relationship between
healthcare personnel and women. B. Women’s knowledge-power.
Trust relationship between staff and women (Figure 1A)
Building links between healthcare personnel and women requires
trust. This allows a therapeutic link to be established where women accept the
recommendations of the staff and there is adherence to the initiatives of the
health services. Confidence changes according to the aspects developed in Table 3.
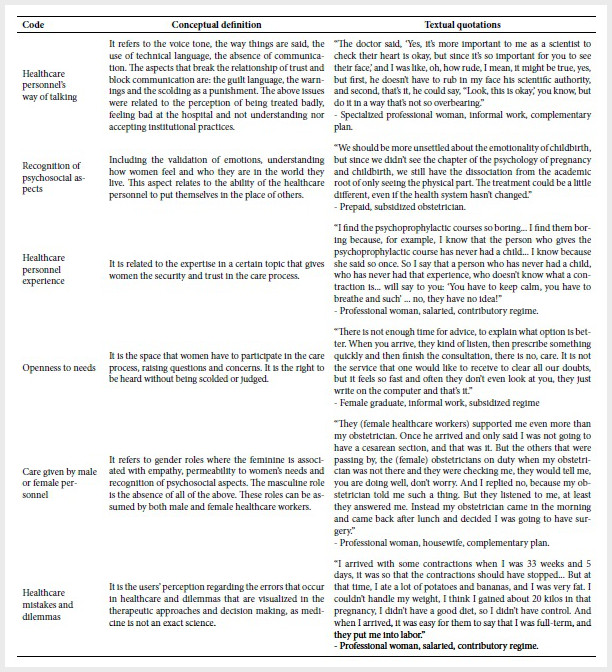
Table 3. Trust relationship category codes between
healthcare personnel and women
The participant observation showed that several
sexual and reproductive rights were violated in all the women participants,
which implies that obstetric and gender violence affects different social
classes. However, for women with a lower social class there are problems that
are intensified to a greater extent. For example, the lack of openness to the
needs of women and the lack of recognition of psychosocial aspects. In this
regard, the healthcare personnel treated the participants as if they were
ignorant and careless regarding their own PLP process. Women are scolded and
judged when medical protocols are not followed. The social context is not taken
into account since they are women who live in the most vulnerable localities of
Bogota and with few social networks (Table 1A), which reduces the use of
healthcare services. The pain in childbirth, breastfeeding, and medical
procedures is naturalized by healthcare personnel and there are no alternatives
to connect with women’s feelings.
Women’s knowledge-power (Figure 1B)
Women possess knowledge that they have built into their life
stories, through the social networks
that surround them and in health services. The way in
which this knowledge is constructed determines the power and decisions they
make in health institutions. The aspects related to this category are
developed in Table 4.
Table 4.
Women’s Knowledge-Power
Category Codes

Inequalities according to social class in the above aspects
include having different points of view
when faced with a medical recommendation and the right
to complain or demand for improvement. In these aspects, women with a lower
social class are affected more. In this regard, the participant observation
showed that the participants did not express their dissatisfaction with the
care provided, nor did they structure formal complaints in the health services.
When discussing this aspect with the women, they expressed fear of
confrontation and their rights acquired a connotation in favor of public
institutions. Similarly, there is a deficit of inputs and human talent in these
services, reducing the alternatives for choosing personnel trained in humane
practices.
DISCUSSION
The findings showed changes in the doctor-patient relationship,
taking into account that it is a social and intersubjective interaction, and it
results from its own socio-political context. There are structural factors that
determine the functioning of health systems under the concept of supply and
demand in the global market (25). The doctor-patient relationship
includes technological elements such as the use of the computer, which is
relevant for the registration of data and acquires a value above the
interaction of the subjects. Likewise, the relationship with the power of the
administrative sector is visible, which diminishes the freedom of the
professional to respond to the market economy, subordinating the ethics of the
healthcare personnel (25). In this research, this problem is part of the
structural barriers that institutions face in applying humanized practices in
PLP.
In this context, the relationship between subjects
is not important, but rather the results expected from the medical act.
Technology is also transformed, since it is no longer an aid but is central to
the structure of medicine. All of the above is more important than the patient,
and medical work becomes dehumanized in a socio-political context that
encourages this problem (25). In this research, technology acquires
a more important role than the signs and symptoms, and also than the accompaniment,
when it comes to physiological and natural childbirth.
The patient-doctor relationship is eliminated by
the institutional administrative agenda which is more important than the
doctor-patient agenda. In this context, care is depersonalized, and meetings
are automated. The doctor’s agenda is structured on the basis of the spatial
and temporal conditions of the medical practice. The space and time of this
consultation is defined by the institution from an administrative framework
that seeks to make medical management profitable. The doctor arrives in a space
for which he prepares in his medical training and is forced to apply his
biomedical knowledge in difficult conditions, since the time of consultation
and the administrative activities that he has to carry out by institutional
order eliminate the possibility of taking into account the socio-cultural
aspects of the HDP (26).
With regard to male and female identities, medicine
has historically been masculinized. This is visualized in the discourse of the
English medical society in the 17th century, where professionals are advised to
avoid contact and intimacy with patients. In the 19th century, the concept of
sympathy (understood as affinity between people who are attracted to each
other) is identified in Victorian society as feminine and unscientific, as are
doctor-patient relationships. In the United States, after graduating, some
doctors integrated sympathy into their work, but others advocated more in favor
of technology and separation from interpersonal relationships. These aspects
have influenced the fact that in the 20th century, sympathy, defined as skills
of an affective nature, has also lost its scientific value (27).
Ignorance of the history of the medical profession
allows this masculinization to persist today and the difficulties in integrating
theoretical and practical knowledge are understandable (27),
which affects the healthcare for health service users, since they transit
through health institutions where healthcare personnel work individually.
Violence against women in PLP has its origins in
medical training, where there are hidden agendas that are learned historically
in academic settings. There is a disassociating habitus on the part of
healthcare personnel who ignore the human character of women during labor, so
it is possible that disrespectful behaviors are validated. The authoritarian
habitus generates threats against women who do not follow medical orders,
blaming them when they do not “collaborate” (call for the norm) in the delivery
process and disqualifying the pain they feel. In the habitus in action, women
are seen as inferior from the professional and gender point of view, which is
relevant for the repressive rules that women accept in a subordinate way in a
context where suffering is supposed to be deserved and the social reality of
the population is ignored (28).
Gender related issues are observed across social
institutions (29) and health
services are no exception (30). In them, the related feminine and
masculine roles are established, giving an account of the hierarchies developed
at a social level (29,30). Women’s partners, present in the research, are
excluded from the care process, assigning the reproductive role exclusively to
women. However, men are included in the services when it is desired to impose
certain institutional practices on women. Autonomy in decision-making about
women’s bodies is determined by the presence of the child, in which the state,
health professionals and the father of the fetus play important roles.
Within the limitations, this research did not seek
to generalize as population studies traditionally do, but rather to understand
specific aspects of the problems raised in the research. A traditional
ethnography was not carried out, where the researcher lives permanently in the
field, but 13 months of observation were carried out, staying in the field at
least three days a week. The participant observation was carried out only by
the principal investigator, taking into account economic limitations. This researcher
is not an anthropologist, but a doctor from Bogota, who is part of the context,
and her vision could ignore other aspects that could be relevant in the
analysis of the information. However, this public health research has been a
collaborative work, where the support of social science researchers was
relevant, who helped to build a comprehensive vision of the medical issues to
be analyzed. It would have been possible for a greater number of people to
participate, in search of the excessive amount of information in relation to
social class, but given the established budget and schedule, more women could
not be invited to participate.
In conclusion, it is necessary to develop
interventions in educational and health institutions that take into account the
theoretical and methodological proposals of this research and the
democratization of medical information. Health inequalities and inequities are
preventable through public policies with a gender perspective that contribute
to transforming both the health and educational systems in Colombia. It is
necessary to study in depth the impact of the HDP on the quality of the care
process and to identify the different masculinities that play important roles
in women’s relationships with healthcare personnel.
Acknowledgements:
To the women and healthcare personnel who participated in the research. Fundación Arka, Organización Apapachoa, Movimiento Nacional por la Salud Sexual y Reproductiva en Colombia, Tribu Criarte, Secretaría de Salud Bogotá. To Marcelo Amable, Alfredo Maya and Monica Saenz for their contributions from the social sciences. To Universidad CES in Medellin and Colciencias for their funding.
REFERENCES
1.
Downe
S, Lawrie TA, Finlayson K, Oladapo OT. Effectiveness of respectful care
policies for women using routine intrapartum services: a systematic review.
Reproductive health. 2018;15(1):23. doi: 10.1186/s12978-018-0466-y.
2.
Organización
Mundial de la Salud. Prevención y erradicación de la falta de respeto y el
maltrato durante la atención del parto en centros de salud [Internet] Ginebra OMS; 2014 [citado 30 de
Enero de 2020]. Disponible en : https://apps.who.int/iris/bitstream/handle/10665/134590/WHO_RHR_14.23_spa.pdf;jsessionid=8D5556D17EF46062AA6DDB21F34094F4?sequence=1.
3.
Monroy
MSA. El continuo ginecobs-tétrico .Experiencias de violencia vividas por
mujeres gestantes en servicios de salud en Bogotá [Tesis maestría]. Bogotá:
Escuela de estudios de Genero Universidad Nacional de Colombia; 2012.Disponible
en: http://www.bdigital.unal.edu.co/7805/1/soniaandreamonroymu%C3%B1oz.2012.pdf.
4.
Briceño
Morales X, Enciso Chaves LV, Yepes Delgado CE. Neither Medicine Nor Health Care
Staff Members Are Violent By Nature: Obstetric Violence From an Interactionist
Perspective. Qualitative health research. 2018;28(8):1308-19. doi: 10.1177/1049732318763351.
5. Vallana Sala VV. Parirás con dolor, lo embarazoso de la práctica obs-tétrica. Discursos y prácticas que naturalizan la violencia obstétrica en Bogotá [Tesis de maestría]. Bogotá: Facultad de Ciencias Sociales. Pontificia Universidad Javeriana; 2016. Disponible en: https://repository.javeriana.edu.co/bitstream/handle/10554/19135/VallanaSalaVivianaValeria2016.pdf?sequence=1&isAllowed=y.
6. Colón IC. Sentimientos, memorias y experiencias de las mujeres en trabajo de parto el caso de centros hospitalarios en Cartagena [Tesis de maestría]. Cartagena: Escuela de estudios de Genero Universidad de Cartagena y Nacional de Colombia; 2008. Disponible en: http://bdigital.unal.edu.co/53287/1/.candelariacoloniriarte.2008.pdf.
7.
Rocha-Acero ML, Socarrás-Ronderos F, Rubio-León DC. Prácticas de atención del
parto en una institución prestadora de servicios de salud en la ciudad de
Bogotá. 2019;37(1):53-65. doi: 10.17533/udea.rfnsp.v37n1a10.
8.
Jojoa-Tobar E, Cuchumbe-Sánchez YD, Ledesma-Rengifo JB, Muñoz-Mosquera MC,
Suarez Bravo JP. Violencia obstétrica: haciendo visible lo invisible. Rev Univ
Ind Santander Salud. 2019;51(2):136-47. doi: http://dx.doi.org/10.18273/revsal.v51n2-2019006.
9.
Bedoya-Ruiz LA, Agudelo-Suárez AA. Relación de las mujeres en embarazo, parto y
postparto (EPP) con los servicios de salud según la clase social. Rev Gerenc
Polít Salud. 2019;18(36). doi: 10.11144/Javeriana.rgps18-36.rmep.
10.
Breilh J. Las categorías causalidad y clase social como elementos de la
ideología epidemiológica. En: Breilh J, editor. Crítica a la interpretación
capitalista de la Epidemiología Un ensayo de desmitificación del proceso de
salud y enfermedad. Méjico: Universidad Autonoma Metropolitana; 1977. P. 78-90.
11.
Breilh J. Breve recopilación sobre operacionalización de la clase social para
encuestas en la investigación social. En: Centro de estudios y asesoría en
salud (CEAS), editor. Quito: Ecuador Centro de estudios y asesoría en salud (CEAS);
1989. p. 1-12.
12.
Menéndez EL. El modelo médico hegemónico. Estructura función y crisis. En:
Menéndez EL, editor. Morir de Alcohol: Saber y Hegemonía Médica. Mexico DF:
Alianza Editorial Mexicana; 1990. p. 83-117.
13.
Menéndez E.L. El punto de vista del actor: homogeneidad, diferencia e
historicidad. En: Menéndez E.L, editor. La parte negada de la cultura:
relativismo, diferencias y racismo. Barcelona: Edicions Bellaterra; 2002. p.
291-365.
14.
Grondin J. Que es la interpretación. En: Grondin J, editor. El Legado de la
Hermeneutica Primera ed. Cali: Universidad del Valle; 2009. p. 15-36.
15.
Packer M. La investigación enmancipadora como reconstrucción racional En:
Packer M, editor. La ciencia de la investigación cualitativa. Bogota,
Universidad de los Andes: Facultad de Ciencias Sociales; 2013. p. 337-363.
16.
Kincheloe J, McLaren P. Replanteo de la teoria critica y de la investigación
cualitativa. En: Denzin NK, Lincoln YS,
editores. Manual de investigación cualitativa Volumen II Paradigmas y perspectivas
en disputa. Barcelona: Gedisa; 2012. p. 241-91.
17.
Scheper-Hughes N. Nervoso. En:
Scheper-Hughes N, editor. La muerte sin
llanto Violencia y vida cotidiana en Brasil. Barcelona: Ariel; 1997. p.
167-212.
18.
Mendizabal N. Los componenentes del diseño flexible en la investigación
cualitativa. En: Vasilachis de Gialdino, editor. Estrategias de investigación
cualitativa. Barcelona: Gedisa; 2006. p. 65-103.
19.
Galeano ME. Diseño de proyectos en la investigación cualitativa: Fondo
Editorial Universidad EAFIT; 2004. p. 11-81.
20.
Organización Panamericana de la Salud. Perfil sistema de salud en Colombia.
[Internet] Washington, D.C: Organización Panamericana de la Salud; 2010 [citado
30 de enero de 2020]. Disponible en : https://www.paho.org/hq/dmdocuments/2010/Perfil_Sistema_Salud-Colombia_2009.pdf?ua=1.
21.
Restrepo ODA. Vigencia de la categoría clase social en salud pública. En:
Estrada M J H, editor. Teoria Critica de la Sociedad y Salud Publica. Bogotá:
Universidad Nacional de Colombia. Universidad de Antioquia; 2011. p. 134-44.
22.
Fontana A, Frey JH. La entrevista. En: Denzin N, Lincoln Y, editores. Manual de
Investigación Cualitativa Volumen IV Métodos de recolección y análisis de
datos. Barcelona: Gedisa, 1ª edición; 2015. p. 140-189.
23.
Evens TMS, Handelman D. Introduction: The Ethnographic Praxis of the Theory of
Practice. Social Analysis [Internet] Brooklyn NY: The International Journal of
Social and Cultural Practice; 2005 [citado el 30 de Enero de 2020]. Disponible
en :
www.jstor.org/stable/23179071.
24.
Strauss A, Corbin J. Bases de la investigación cualitativa. Técnicas y
procedimientos para desarrollar la teoría fundamentada. Medellin: Editorial
Universidad de Antioquia Facultad de Enfermería de la Universidad de Antioquia;
2002 .p. 3-197
25.
Rossi I. Capítulo 2. La clínica como
espacio social. Época de cambios o cambio de época?. En: Hamui Sutton L, Maya A
P, Hernández Torres I, editores. La comunicación dialógica como competencia
médica esencial. Ciudad de Mexico: Manual Moderno; 2018. p. 38-58.
26.
Cruz Sanchez M, Hernández Torres I, Grijalva MG, Maya A P, Dorantes P. Capitulo
3. El ejercicio de la profesión médica y la comunicación médico paciente en
contextos situacionales. En: Hamui Sutton L, Maya A P, Hernández Torres I,
editores. La comunicación dialógica como competencia médica esencial. Ciudad de
Mexico: Manual Moderno; 2018. p. 58-100.
27.
Ortiz G T. El género, organizador de profesiones sanitarias. En: Miqueo C,
Tomas C, Tejero C, Barral M J, Fernandez T, Yago T, editors. Perspectivas de
Género en Salud Fundamentos Científicos y Socioprofesionales de Diferencias
Sexuales No Previstas. Madrid: Minerva Ediciones, S.A; 2001. p. 53-77.
28.
Castro R. El habitus en acción. La atención autoritaria del parto en los
hospitales. En: Castro R, Ervite J editores. Sociología de la práctica médica
autoritaria. Violencia obstetrica, anticoncepción inducida y derechos
reproductivos. Cuernavaca, Mexico: Universidad Nacional Autonoma de Mexico;
2015. p. 81-131.
29.
Connell R, Pearse R. Gender theorist and gender theory. En: Connell R, Pearse
R, editors. Gender In world perspective 3rd ed. Cambridge: Polity Press; 2015.
p. 68-206.
30.
Lorber J, Moore LJ. Hierarchies in helath care: patients, professionals and
gender. En: Lorber J, Moore LJ, editors. Gender and the social construction of
illnes. Lanham: Altamira Press; 2002. p. 37-51.
Sources of funding: Colciencias National Doctoral Scholarship calling 647-2014 and Small Amount Calling from Universidad CES in Medellin, Colombia.
Citation: Bedoya-Ruiz LA, Agudelo-Suarez AA, Restrepo-Ochoa DA. Relations
established by women during pregnancy, delivery and postpartum with health
personnel according to social class in bogotá: qualitative study. Rev Peru Med
Exp Salud Publica. 2020;37(1):
7-16. Doi:
https://doi.org/10.17843/rpmesp.2020.371.4963
Correspondence to:
Libia A. Bedoya-Ruiz; Escuela de Graduados, Universidad CES,
Medellin, Colombia; Calle 10 A No. 22 – 04. Medellin, Colombia;
bedoya.libia@ces.edu.co,
bedoyalibia@hotmail.com.
Authors’ contributions:
All
authors participated in the conception, design of the work, analysis, data
interpretation, critical review and approval of the final version. LABR carried
out the data collection and initial writing of the article. All authors are
responsible for all aspects of the manuscript and warrant its content. This
article is part of LABR’s doctoral training process in the PhD in Public Health
at Universidad CES and will be used as part of the material used for the thesis
dissertation.
Conflicts of interest:
All authors declare that they have no conflict of interest.
Received:
14/11/2019
Approved:
05/02/2020
Online:
23/03/2020