Rodrigo M. Carrillo-Larco
Antonio Bernabé-Ortiz
Original article
Prevalence and incidence of arterial hypertension in peru: a systematic review and meta-analysis
Andrea Ruiz-Alejos ![]() 1,2, Physician, Master in Public Health, Doctor in Epidemiology
1,2, Physician, Master in Public Health, Doctor in Epidemiology
Rodrigo M. Carrillo-Larco ![]() 1,3, Physician
1,3, Physician
Antonio Bernabé-Ortiz ![]() 1,4, Physician, Master in Public Health, Doctor in Epidemiology
1,4, Physician, Master in Public Health, Doctor in Epidemiology
1 CRONICAS Centro de Excelencia en Enfermedades Crónicas, Universidad Peruana Cayetano Heredia, Lima, Peru.
2 Facultad de Ciencias de la Salud, Universidad Peruana de Ciencias Aplicadas, Lima, Peru.
3 Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, London, UK.
4 Universidad Científica del Sur, Lima, Peru.
ABSTRACT
Objective. To determine the prevalence and incidence of arterial hypertension, as well as the prevalence of previous diagnosis of arterial hypertension (self-reported) among the adult population of Peru.
Materials and methods. Systematic review and meta-analysis of epidemiological studies available in LILACS, EMBASE, MEDLINE and Global Health. Studies were included if they followed a random sampling approach in adult population. Screening and assessment of manuscripts was carried out independently by two researchers. A random-effects meta-analysis was conducted to quantify the overall prevalence and incidence of hypertension. The Newcastle-Ottawa scale was used to assess the risk of bias in the manuscripts.
Results. A total of 903 papers were screened, and only 15 were included in the estimation of hypertension prevalence, 8 in the assessment of previous hypertension diagnosis, and 4 for incidence estimations. The pooled prevalence of hypertension was 22.0% (95% CI: 20.0% - 25.0%; I2=99.2%). This estimate was lower in national studies [20.0% (95% CI: 17.0% - 22.0%; I2=99.4%] than in sub-national studies [24.0% (95% CI: 17.0% - 30.0%; I2=99.2%]. The pooled prevalence of previous hypertension diagnosis was 51.0% (95% CI: 43.0% - 59.0%; I2=99.9%). The pooled incidence of hypertension was 4.2 (95% CI: 2.0 - 6.4; I2=98.6%) per 100 person-years. The included studies did not present high risk of bias.
Conclusions. Our findings show that one in five Peruvians has hypertension, and that four new cases appear per 100 persons per year; in addition, only half of the subjects with hypertension are previously diagnosed.
Keywords: Hypertension; Undiagnosed Hypertension; Systematic Review; Meta-analysis; Prevalence; Incidence; Peru (source: MeSH NLM).
INTRODUCTION
Arterial hypertension (HT) is considered as the leading cause of preventable mortality worldwide (1). HT affects more than 1 billion people worldwide, mostly those in low- and middle-income countries (2). Self-reported HT may be the cause for low diagnosis rates, which contributes to the increase in complications due to this condition in underdeveloped countries (3). Moreover, 10% of global healthcare expenses are allocated only to the treatment of identified cases, reaching up to one trillion US dollars with suboptimal treatment (4).
Population-based studies in middle- and low-income countries have shown an increased prevalence of HT compared to high-income countries, where there is a sustained decrease (2,5). However, recent data have shown contradictory trends, especially in South America and the Caribbean, where the prevalence of HT is stable or decreasing (3). A recent Peruvian study on trends in prevalence and treatment of hypertension reported that the age-standardized prevalence of hypertension increased from 18.7% in 2015 to 20.6% in 2018, whereas the prevalence of previous diagnosis and control of this condition decreased (6). Accordingly, in 2018, less than half of hypertensive Peruvians were diagnosed; 20.6% were receiving treatment, and only 5.3% had adequate control. Likewise, it was evidenced that the lowest proportions of diagnosis, treatment, and control of HT were in people living in rural areas and with low socioeconomic status (6).
The available literature on HT is mostly focused on prevalence, but not on the percentage of previously diagnosed HT, much less on the incidence of this condition. Knowledge of the prevalence of hypertension in Peru, as well as previous diagnosis and incidence, is limited to studies in certain sectors and/or population groups that may not reflect the true situation of HT in the country. To date, there is only one narrative review of arterial hypertension in Peru, describing studies that are not representative of the general population (7). As a consequence, the main objective of this study was to conduct a systematic review and meta-analysis of population-based studies of prevalence, incidence, and previous diagnosis of HT in Peru. In this way, we will have combined estimates of these epidemiological indicators necessary for the development of HT control policies in our context.
|
KEY MESSAGES |
|
Motivation for the study: The available literature on hypertension is focused on prevalence, but not on the proportion of those with a previous diagnosis, much less on the incidence of this condition in Peru. Main findings: The aggregate prevalence of hypertension was 22.0%, slightly higher in males (24.0%) than in females (23.0%). This prevalence was 20.0% in national studies and 24.0% in subnational studies. The proportion of subjects with a previous diagnosis of hypertension was 51.0%. The incidence of hypertension was 4.2 per 100 person-years of follow-up. Implications: Our findings suggest the need for a hypertension surveillance and prevention system in Peru. |
MATERIALS AND METHODS
Study design
The present study is based on a systematic review and meta-analysis of the literature to synthesize the available scientific information on the prevalence and incidence, and secondarily, the proportion of subjects with a previous diagnosis of HT in Peru. The PRISMA (8,9) methodology was used for this purpose.
Selection criteria
We selected population-based studies, representative of the general adult population (18 years and older) and with probability sampling (random selection of participants). We included studies that presented the outcome of interest, that is, prevalence and/or incidence of hypertension. Only studies conducted in Peru that included the Peruvian population residing in Peru were included; therefore, those with a foreign population or Peruvians residing in other countries were excluded. The studies had to have at least two blood pressure measurements and had to define HT according to the Joint National Committee (JNC-8) (10), which considers HT based on measurement, self-report of disease, and/or antihypertensive treatment.
Secondarily, we included studies that reported a previous diagnosis of the disease when the data was described or could be obtained from the information available in the manuscript. However, this was only the case if the manuscript had data on the prevalence of arterial hypertension. Studies based on case reports or case series, or in a specific population (hospital sample or belonging to a specific institution, subjects with metabolic syndrome or overweight) were excluded.
Sources of information
OVID and LILACS (Latin American and Caribbean Health Sciences Literature) were the databases we consulted. OVID included EMBASE, MEDLINE and Global Health databases; LILACS was considered for its large number of Latin American studies published in journals not indexed in other databases.
Search strategy
The search for studies was conducted on January 14, 2021. No additional restrictions (e.g. language) or date limits were considered. Details on the terms used in each search engine are presented in Supplementary Table 1.
Table 1. Characteristics of the studies included for the prevalence analysis.
|
Author and year |
Name of the study |
Year of recollection |
Scope |
Sample size |
Proportion of women |
Age average |
|
Seclen S. (1999) |
|
- |
Subnational |
598 |
68.1 |
40.4 |
|
Goldstein J. (2005) |
|
1998-2000 |
Subnational |
2,337 |
49.9 |
40.1 |
|
Medina-Lezama J. (2007) |
PREVENCION |
- |
Subnational |
1,878 |
53.8 |
49 |
|
Hernández-Hernández R. (2010) |
CARMELA |
2003-2005 |
Subnational |
1,652 |
53.4 |
43.6 |
|
Prince M.J. (2012) |
10/66 |
2003-2005 |
Subnational |
1,929 |
61.2 |
74.8 |
|
Lerner A. (2013) |
PERU MIGRANT |
2007 |
Subnational |
987 |
52.8 |
48 |
|
Heitzinger K. (2014) |
|
2012 |
Subnational |
142 |
69.7 |
35.9 |
|
Romero C. (2014) |
|
2008 |
Subnational |
76 |
52.6 |
47.4 |
|
Arribas-Harten C. (2015) |
ENDES |
2013 |
National |
4,641 |
53.6 |
37.1 |
|
Irazola V. (2016) |
CRONICAS |
2010-2012 |
Subnational |
2,918 |
51.9 |
- |
|
Taype-Rondan A. (2017) |
CRONICAS |
2013-2014 |
Subnational |
2,433 |
51.3 |
57.2 |
|
Geldsetzer P. (2019) |
WHO STEPS |
2012 |
Subnational |
29,415 |
52.6 |
61 |
|
Barboza E. (2020) |
|
2018 |
Subnational |
412 |
- |
- |
|
Bernabé-Ortiz A. (2020) |
SALT |
2014 |
Subnational |
2,376 |
50.4 |
43.3 |
|
|
ENDES |
2015 |
National |
27,412 |
51.1 |
- |
|
Villarreal-Zegarra D. (2020)a |
ENDES |
2016 |
National |
26,680 |
50.9 |
- |
|
|
ENDES |
2017 |
National |
27,142 |
51.6 |
- |
|
|
ENDES |
2018 |
National |
28,167 |
51.7 |
- |
a Because of the national scope and annual prevalence analysis, four different studies were considered.
Selection of studies
At the end of the search, we downloaded the results, then the title and abstract of each article were screened and duplicates were eliminated (first phase). In addition, conference abstracts and manuscripts unavailable because of their age were excluded. Then, we downloaded and critically read the full text of the selected articles, then the selection criteria were applied (second phase). In both phases, screening was carried out independently by two researchers (AR-A and AB-O). In cases of conflict, these were resolved by agreement of both researchers or by intercession of another researcher author of this study (RMC-L). Rayyan software was used to carry out the two screening phases (11).
Since the final result of the search could include more than one article per study, all relevant information was extracted from each article. This process was carried out by the same reviewers as in the first phases, independently, and then the selection of articles was discussed. The criteria used for the selection of articles from the same research study were as follows: 1) the main objective of the study was to estimate the prevalence or incidence of hypertension; 2) the article with the largest sample size; and 3) the article with the most information in addition to the prevalence or incidence of hypertension (for example, data on previous diagnosis of hypertension and an estimate of the prevalence of hypertension according to sex). Because several studies used data from the National Demographic and Health Survey (ENDES), conducted annually, the data on HT prevalence were considered for each year individually; that is, they were analyzed as different studies. Furthermore, in only one case we included
two studies from the same cohort, since each conducted a cross-sectional analysis of two different time intervals and one provided data on previous diagnosis.
Extraction of information
The information relevant to the review was extracted using a data form specially prepared by the authors of this article. For prevalence studies, the form included the following data: first author, name of the study, year of publication, year of data collection, study design, scope of the study (national or subnational), reported sample size, percentage of women in the sample, mean age of the study sample, operational definition of hypertension, prevalence of hypertension in the total sample, prevalence of disease awareness, and prevalence of hypertension by sex.
In the case of incidence studies, the form included the first author, name of the study, year of publication, year of data collection at the start of enrollment, scope of the study (national or subnational), sample size at the start of enrollment, operational definition of hypertension, type of incidence assessed, number of new cases, cohort follow-up years (in person-years), and overall incidence of hypertension. Data extraction was conducted in duplicate. Two authors (AR-A and AB-O) extracted the information from each study to contrast and verify their accuracy.
Risk of bias
An adapted version of the Newcastle-Ottawa scale was used for cross-sectional studies (12). On the other hand, the original criteria of the Newcastle-Ottawa scale were used to assess the risk of bias in cohort-type articles (13). The assessment was made independently by two researchers (AR-A and AB-O), any conflicts were resolved by consensus or by a third study author (RMC-L). For both cases, low risk of bias was defined as those studies that, according to the five areas evaluated, had A or B grades in all scores, while high-risk studies were those that included at least a C, D or E classification. This was done to facilitate sensitivity analysis according to risk of bias.
Synthesis and analysis
Statistical analysis was conducted using STATA v.16 for Windows (StataCorp, College Station, TX, US). Initially, we conducted a qualitative description of the studies included in the review.
Then, a quantitative analysis (meta-analysis) was conducted for each of the variables of interest in the study: prevalence of hypertension and disease awareness, and incidence of hypertension. For the estimation of proportions (prevalence of hypertension and those with a previous diagnosis), we obtained the pooled estimate after the stabilization of variances using the Freeman-Tukey transformation (14). Because of the expected high heterogeneity, the meta-analysis was conducted using a random-effects model based on the method of DerSimonian and Laird (15), and the pooled estimate of prevalence and their respective 95% confidence intervals (95% CI) were obtained. This procedure was valid for estimating the aggregate prevalence of hypertension (overall and by sex), as well as for sensitivity analysis (according to mean study age, scope, year of data collection, sample size, and risk of bias) and the proportion of those with a previous diagnosis (expressed as total subjects with hypertension). I2 was used to quantify heterogeneity. Random-effects meta-regression models were run using the variables extracted and presented in the descriptive tables to determine potential factors associated with such heterogeneity.
For the estimation of the pooled incidence, we calculated the estimate per person-year. As for prevalence, we estimated the incidence rate per 100 person-years of follow-up and their respective 95% CIs.
RESULTS
Selection of studies
From the initial search in OVID and LILACS, 962 titles and abstracts were found, of which 59 duplicates were eliminated, resulting in 903 titles and abstracts. After screening, only 47 articles were selected for full-text download. From these 47, the most representative article of each study was extracted and selected according to the previously defined criteria. Finally, fifteen manuscripts were selected for prevalence calculation (n = 161,195) (6,16-28); eight manuscripts were used for estimation of prevalence of previous HT diagnosis (n =118,983) (6,18-23,25), and three of the four available manuscripts (26,29-31) for incidence calculation (n = 6116). Details of article exclusion in each phase are illustrated in Figure 1.
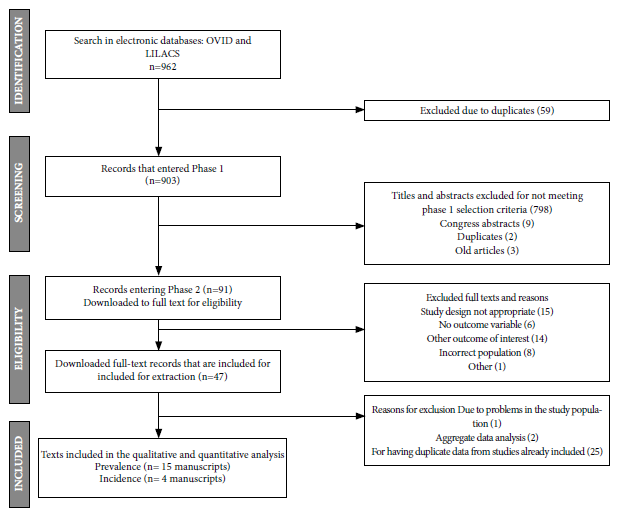
Figure 1. Flowchart of the selection of studies included in the present
Characteristics of the studies
In the case of the HT prevalence studies, only four of the fifteen manuscripts were written in Spanish (16,23,24,28). On the other hand, four of the prevalence studies were included as part of an international study (19,20,25,27). The oldest article was published in 1999 (16) and the most recent ones were published in 2020; in two articles the year of data collection could not be obtained. Three articles of national scope were found (6,24,27). The article by Villarreal-Zegarra et al. analyzed 4 consecutive years of ENDES data, so each year was considered as a different study (6). Twelve studies were subnational, included urban and rural populations, and were the baseline of a cohort as in the case of the CRONICAS or PERU MIGRANT cohorts. Detailed information on the studies included in the present review is available in Table 1.
Regarding incidence studies, only four articles were included from the following cohorts: CRONICAS (26), PERU MIGRANT (n = 2) (29,31), and an intervention using a salt substitute in the north of the country (30). All studies were subnational in scope, representative of the cities of Tumbes, Lima, Ayacucho and Puno. As shown in Table 2, the study with the longest follow-up time was the one by Ruiz-Alejos et al. with 6.5 years of the PERU MIGRANT cohort (31); however, the study published by Bernabé-Ortiz et al. based on the CRONICAS cohort (26) reported the highest incidence of HT (7.12 per 100 person-years; 95% CI: 6.44 - 7.88).
Table 2. Characteristics of the studies included for the incidence analysis.
|
Author and year |
Study name |
Year of baseline |
Year of follow-up |
Scope |
Baseline sample size |
Proportion of women |
Mean age |
|
Bernabé-Ortiz A. (2017) |
CRONICAS Cohort |
2010 |
2.4 |
Subnational |
3,237 |
52.6 |
55.8 |
|
Bernabé-Ortiz (2017) |
PERU MIGRANT a |
2007-2008 |
5.2 |
Subnational |
988 |
52.8 |
47.9 |
|
Ruiz-Alejos A. (2020) |
PERU MIGRANT a |
2007-2008 |
6.5 |
Subnational |
988 |
53 |
48 |
|
Bernabé-Ortiz A. (2020) |
Salt substitute study |
2014 |
-- |
Subnational |
1,891 |
49.6 |
43.3 |
a The PERU MIGRANT studies analyze cohort data at different follow-ups, so both were included. Only the study with the longest follow-up was used.
Aggregate prevalence of arterial hypertension.
More than 50% of the studies had two or more blood pressure measurements and calculated the mean of at least two measurements for HT case definition (6,17-19,21-23,25-27,30). Four articles (22% of studies) did not specify the number of blood pressure measurements (16,20,20,24,28); however, these studies detailed that the case definition followed the JNC-8 guideline.
Total prevalence data from 18 studies were included in the meta-analysis. The CARMELA study (19) reported the lowest prevalence (12.6%) while the 10/66 study (20) conducted in older adults (i.e. ≥65 years) found a prevalence of 49.7%. The pooled prevalence was 22.0% (95% CI: 20.0% - 25.0%), but there was high heterogeneity (I2 = 99.2%) (Figure 2).
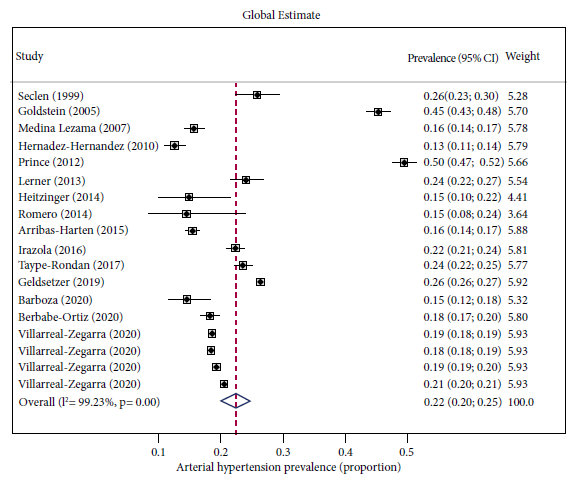
Figure 2. Combined prevalence of arterial hypertension in Peru.
Eleven studies provided data on the prevalence of hypertension by sex. The aggregate prevalence in men was 24.0% (95% CI: 20.0% - 28.0%) (Supplementary Figure 1), whereas a prevalence of 23.0% (95% CI: 17.0% - 28.0) was obtained for women (Supplementary Figure 2). The heterogeneity obtained from the quantitative analyses of the male and female populations remained similar to the analysis of the general population (98.1% and 99.3%, respectively).
As part of the sensitivity analysis, the aggregate prevalence of hypertension was higher in studies with an older mean age: 21% (95% CI: 14% - 28%, I2: 99.0%) in participants <50 years compared with studies with subjects ≥50 years: 33% (95% CI: 21% - 45%, I2: 99.5%). A prevalence of 20.0% (95% CI 17.0% - 22.0%; I2 = 99.4%) was obtained from national studies, whereas the aggregate prevalence from subnational studies (61.1% of studies) was 24.0% (95% CI 17.0% - 30.0%; I2 = 99.2%. Further sensitivity analyses are shown in Figure 3 and in all cases, heterogeneity was high.
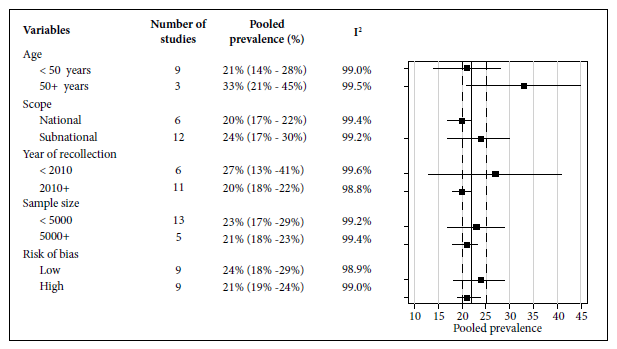
Figure 3. Pooled prevalence of hypertensive disease in Peru: sensitivity analysis.
Eleven studies (6,18-23,25) allowed estimation of the aggregate prevalence of previous diagnosis of hypertensive disease (of the total number of subjects with hypertension) in the general population, which was 51.0% (95% CI 43.0% - 59.0%) with a heterogeneity of 99.9% (Supplementary Figure 3).
Finally, the meta-regression analysis showed that both the year of publication (p = 0.03) and the age of the participants (p = 0.04) had a positive influence on the heterogeneity of the results of the studies analyzed.
Aggregate incidence of arterial hypertension.
On the other hand, given that one study (PERU MIGRANT), had two incidence estimates, both are described in Table 2; however, only the one with the longer follow-up time was the one used for the meta-analysis. Thus, the aggregate incidence resulted in an overall effect of 4.2 (95% CI: 2.0 - 6.4) per 100 person-years of follow-up, with high heterogeneity as in previous analyses (I2 = 98.6%).
Risk of bias
The overall risk of bias of the included studies was low, mainly because they met the study inclusion criteria. Only one study did not specify in detail the definition of blood pressure (Supplementary Table 2). On the other hand, three studies had a partially representative sample or a sample size that was not statistically justified (16,23,28).
DISCUSSION
Regarding hypertension prevalence, and according to the studies included in this systematic review and meta-analysis, it is possible to conclude that at least one in five Peruvians has hypertension. The prevalence of HT ranges between 20 and 25%, being higher in studies that had a subnational scope and that included population from regions with a high prevalence of factors associated with HT such as obesity and type 2 diabetes, in addition to those cities with a high urbanization process such as Lima and Tumbes (21,26,29). The quantitative analysis by sex showed that the prevalence is slightly higher in men than in women. Although there are no studies that analyze the prevalence according to age groups, it is important to highlight that in the study by Prince et al. the prevalence of HT found was almost 50% in those over 65 years of age (20).
On the other hand, about half of hypertensive Peruvians have previous diagnosis of their disease. Villarreal-Zegarra et al. reported inverse trends between prevalence of hypertension and previous diagnosis during the years 2015 to 2018, finding an increase in the prevalence of hypertension from 18.7% to 20.6%, respectively; while the prevalence of previous diagnosis decreased by 10% being 43.5% in 2018 (6). Regarding the incidence of HT, an estimate could only be obtained from three subnational studies, which confirmed the rising trend reported by prevalence studies.
When applying the selection criteria, more than two-thirds of the included studies had a subnational scope. Most of the studies included in the meta-analyses of prevalence and previous diagnosis were representative of less than three cities and/or communities. As such, population scope was the most important limitation of the studies included in the meta-analysis. Nevertheless, they had a low risk of bias and high representativeness.
Considering that the national studies belong to a secondary analysis of the ENDES, applied at the national level, the inclusion of specific areas with good access and available participants can be highlighted. Likewise, it is important to note that there is a lack of studies that address the epidemiological situation of arterial hypertension in Peru, especially prospective studies that analyze the incidence of HT at the national level, or in specific areas such as the jungle, where the evidence is even more limited.
Not all the studies had the same definition of cases of arterial hypertension. In some, only the mean of two blood pressure measurements was considered. Thus, it was to be expected that the variability between studies would be high. This resulted in high heterogeneity levels from the quantitative analysis of estimates in the general population and population subgroups.
Although databases such as LILACS were included, which increased the possibility of finding Peruvian scientific literature, theses or other types of manuscripts that could provide relevant information could have been omitted. However, taking into account the rigorous selection criteria used in this analysis, it is unlikely that there are studies not published in indexed journals that meet the criteria of population representativeness or that contain relevant information at the national level. Likewise, it is to be expected that the theses are limited to captive populations (hospitals, clinics, among other health centers), convenience sampling, or limited sample size, so we believe it is unlikely that the exclusion of these will impact our results. On the other hand, meta-regression showed that much of the existing heterogeneity was secondary to the mean age of the study evaluated, as well as to the year of data collection. The latter could be associated with the increase in the prevalence of hypertension over time.
Our results related to the prevalence of HT show that the preventive management of this disease has not been able to contain the increasing trend of HT cases. Currently, the Ministry of Health guidelines for the management and control of hypertensive disease are focused on detection and prevention in at-risk populations such as men over 55 years of age and women over 65 years of age, diabetic patients, and those obese and overweight. The suggestions in this guideline suggest screening all adults over 18 years of age and follow-up according to blood pressure levels found. However, screening is limited to those who come to the health center, and there are no indications for health personnel to carry out home screening and/or health campaigns.
In addition, the clinical guidelines state that persons with systolic blood pressure <120 and diastolic blood pressure <80 without risk factors would be reevaluated every 5 years. Only in the case of having comorbidity or systolic blood pressure between 120 and 139 or diastolic between 80 and 89 would controls be performed annually. These limitations in the MINSA guidelines could explain the low prevalence of previous diagnosis of disease in adults compared to the population over 65 years of age.
On the other hand, only half of the patients with HT were aware of their diagnosis. The control and treatment of hypertensive disease is directly affected by the timely diagnosis. In high-income countries where high rates of previous diagnosis and control of HT were found, a reduction in prevalence was evidenced (32).
The lack of screening and diagnosis of this disease is reflected in the low percentages of blood pressure control in patients with HT, especially in rural areas and/or low resources (6,21). Villareal-Zegarra et al. found that 5% of patients with HT had controlled blood pressure levels and that sub-analysis in those who reported receiving treatment, control percentages did not exceed 35.4% for 2018, lower than previous years (6). It is worth mentioning that males, despite having a higher prevalence of HT, have the lowest diagnosis rates, according to nationwide studies. This can be explained, in part, by the fact that the screenings and censuses funded (e.g., ENDES) by the Peruvian government are focused on maternal and child health objectives, in addition to the greater willingness of women to participate. In 2019, the ENDES reported a higher percentage of hypertensive women with controlled disease compared to men (70.2 vs. 65.0%) (33). Likewise, the areas with the highest percentage of treatment were Metropolitan Lima and the rest of the coast, which shows the centralization of health resources. Although the Sierra have lower percentages, prospective studies highlight the trend toward an increase in cases of hypertension in this region (29). Training health personnel and community agents in blood pressure measurement (three times) has proven to be effective and with low rejection rates in rural areas (34). Therefore, it is necessary to recognize and rethink intervention and screening strategies that could serve as an opportunity for early detection of HT.
The World Health Organization reported that during 2019, 80% of health expenditures and investment were made in high-income countries (35), being 70 times higher than low-income countries. Peru is one of the countries with the lowest health spending rates worldwide with a health investment of 12.7% for 2019 (36). The 2019 report of the noncommunicable diseases budget program only reported 50.5% of budget execution in this type of pathologies, not considering blood pressure screening but the control and treatment of people already diagnosed, equivalent to 47.3%(37). Considering the limited budget and inadequate management of primary prevention of arterial hypertension, it is necessary to opt for innovative strategies that reduce the gaps of language, access, distance and interculturality. The use of text messages, voice messages, and smartphones has demonstrated improved adherence to treatment and control of HT (38,39), and may be a cost-effective alternative for the control of the epidemiological situation of arterial hypertension in Peru.
In conclusion, the results of the present systematic review confirm a high prevalence and incidence of hypertensive disease in Peru, and that only 50% of the cases with HT have a previous diagnosis of this condition. Studies on the incidence of HT are scarce, being mostly local and not national.
Author contributions: AB-O and RMC-L conceived the research idea. AB-O conducted the search. AB-O and AR-A selected the studies. RMC-L and AB-O performed the study analyses. A-RA wrote the first draft of the article. AB-O and RMC-L performed the critical editing of the article. The three authors accepted the final content of the article and approved this version for publication.
Conflict of interest: None.
Funding: Rodrigo M. Carrillo-Larco is funded by the Wellcome Trust (214185/Z/18/Z).
Supplementary material: Available in the electronic version of the RPMESP.
REFERENCIAS BIBLIOGRÁFICAS
1. GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1923-94. doi: 10.016/S0140-6736(18)32225-6.
2. Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation. 2016;134(6):441-50. doi: 10.1161/CIRCULATIONAHA.115.018912.
3. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet. 2017;389(10064):37-55. doi: 10.1016/S0140-6736(16)31919-5.
4. Gaziano TA, Bitton A, Anand S, Weinstein MC. The global cost of nonoptimal blood pressure. J Hypertens. 2009;27(7):1472-7. doi: 10.097/HJH.0b013e32832a9ba3.
5. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223-37. doi: 10.1038/s41581-019-0244-2.
6. Villarreal-Zegarra D, Carrillo-Larco RM, Bernabe-Ortiz A. Short-term trends in the prevalence, awareness, treatment, and control of arterial hypertension in Peru. J Hum Hypertens. 2020;35(5):462-71. doi: 10.1038/s41371-020-0361-1.
7. Herrera-Añazco P, Pacheco-Mendoza J, Valenzuela-Rodríguez G, Málaga G. [Self-Knowledge, Adherence to Treatment, and Control of Arterial Hypertension in Peru: a Narrative Review]. Rev Peru Med Exp Salud Publica. 2017;34(3):497-504. doi: 10.17843/rpmesp.2017.343.2622.
8. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi: 10.1371/journal.pmed.
9. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021;372:n71. doi: 10.1136/bmj.n71.
10. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). Jama .2014;311(5):507-20. doi: 10.1001/jama.2013.284427.
11. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan - a web and mobile app for systematic reviews. Systematic Reviews. 2016;5:210.
12. Modesti PA, Reboldi G, Cappuccio FP, Agyemang C, Remuzzi G, Rapi S, et al. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS One. 2016;11(1):e0147601. doi: 10.1371/journal.pone.
13. Wells GA, Shea B, O´Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa, Canada: The Ottawa Hospital Research Institute; 2021 [updated 2021; visitado 2021 April 23]; Disponible en: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
14. Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Satist. 1950;21(4):607-11. doi: 10.1214/aoms/1177729756.
15. DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. 2015;45(Pt A):139-45. doi: 10.1016/j.cct.2015.09.002.
16. Seclén Santisteban S, Leey Casella J, Villena Pacheco AE, Herrera Mandelli BR, Menacho J, Carrasco A, et al. Prevalencia de obesidad, diabetes mellitus, hipertensión arterial e hipocolesterolemia como factores de riesgo coronario y cerebrovascular en población adulta de la Costa, Sierra y Selva del Perú. Acta Med Peru. 1999;17(1):8-12.
17. Goldstein J, Jacoby E, del Aguila R, Lopez A. Poverty is a predictor of non-communicable disease among adults in Peruvian cities. Prev Med. 2005;41(3-4):800-6. doi: 10.1016/j.ypmed.2005.06.001.
18. Medina-Lezama J, Zea-Diaz H, Morey-Vargas OL, Bolaños-Salazar JF, Postigo-Macdowall M, Paredes-Díaz S, et al. Prevalence and patterns of hypertension in Peruvian Andean Hispanics: the PREVENCION study. J Am Soc Hypertens. 2007;1(3):216-25. doi: 10.1016/j.jash.2007.02.003.
19. Hernández-Hernández R, Silva H, Velasco M, Pellegrini F, Macchia A, Escobedo J, et al. Hypertension in seven Latin American cities: the Cardiovascular Risk Factor Multiple Evaluation in Latin America (CARMELA) study. J Hypertens. 2010;28(1):24-34. doi: 10.1097/HJH.0b013e328332c353.
20. Prince MJ, Ebrahim S, Acosta D, Ferri CP, Guerra M, Huang Y, et al. Hypertension prevalence, awareness, treatment and control among older people in Latin America, India and China: a 10/66 cross-sectional population-based survey. J Hypertens. 2012;30(1):177-87. doi: 10.1097/HJH.0b013e32834d9eda.
21. Lerner AG, Bernabe-Ortiz A, Gilman RH, Smeeth L, Miranda JJ. The "rule of halves" does not apply in Peru: awareness, treatment, and control of hypertension and diabetes in rural, urban, and rural-to-urban migrants. Crit Pathw Cardiol. 2013;12(2):53-8. doi: 10.1097/HPC.0b013e318285ef60.
22. Heitzinger K, Montano SM, Hawes SE, Alarcón JO, Zunt JR. A community-based cluster randomized survey of noncommunicable disease and risk factors in a peri-urban shantytown in Lima, Peru. BMC Int Health Hum Rights. 2014;14:19. doi: 0.1186/472-698X-14-19.
23. Romero C, Zavaleta C, Cabrera L, Gilman RH, Miranda JJ. [High blood pressure and obesity in indigenous Ashaninkas of Junin region, Peru]. Rev Peru Med Exp Salud Publica. 2014;31(1):78-83.
24. Arribas-Harten C, Battistini-Ugarte, T, Rodriguez-Teves MG, Bernabe-Ortiz A. Asociación entre obesidad y consumo de frutas y verduras: un estudio de base poblacional en Perú. Rev Chil Nutr. 2015;42(3):241-7. doi: 10.4067/S0717-75182015000300003.
25. Irazola VE, Gutierrez L, Bloomfield G, Carrillo-Larco RM, Dorairaj P, Gaziano T, et al. Hypertension Prevalence, Awareness, Treatment, and Control in Selected LMIC Communities: Results From the NHLBI/UHG Network of Centers of Excellence for Chronic Diseases. Glob Heart. 2016;11(1):47-59. doi: 10.1016/j.gheart.2015.12.008.
26. Taype-Rondan A, Abbs ES, Lazo-Porras M, Checkley W, Gilman RH, Smeeth L, et al. Association between chronic conditions and health-related quality of life: differences by level of urbanization in Peru. Qual Life Res. 2017;26(12):3439-47. doi: 10.1007/s11136-017-1649-7.
27. Geldsetzer P, Manne-Goehler J, Marcus ME, Ebert C, Zhumadilov Z, Wesseh CS, et al. The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. Lancet. 2019;394(10199):652-62. doi: 10.1016/S0140-6736(19)30955-9.
28. Barboza Palomino EE. Prevalencia de factores de riesgo para enfermedades crónicas no transmisibles en Perú. Rev Cuid. 2020;11(2):e1066. doi: 10.15649/cuidarte.1066.
29. Bernabe-Ortiz A, Sanchez JF, Carrillo-Larco RM, Gilman RH, Poterico JA, Quispe R, et al. Rural-to-urban migration and risk of hypertension: longitudinal results of the PERU MIGRANT study. J Hum Hypertens. 2017;31(1):22-8. doi: 10.1038/jhh.2015.124.
30. Bernabe-Ortiz A, Sal y Rosas VG, Ponce-Lucero V, Cárdenas MK, Carrillo-Larco RM, Diez-Canseco F, et al. Effect of salt substitution on community-wide blood pressure and hypertension incidence. Nat Med. 2020;26(3):374-8. doi: 10.1038/s41591-020-0754-2.
31. Ruiz-Alejos A, Carrillo-Larco RM, Miranda JJ, Gilman RH, Smeeth L, Bernabé-Ortiz A. Skinfold thickness and the incidence of type 2 diabetes mellitus and hypertension: an analysis of the PERU MIGRANT study. Public Health Nutr. 2020;23(1):63-71. doi: 10.1017/S1368980019001307.
32. NCD Risk Factor Collaboration (NCD-RisC). Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet 2019;394(10199):639-51. doi: 10.1016/S0140-6736(19)31145-6.
33. Instituto Nacional de Estadística e Informática. Peru: Enfermedades transmisibles y no transmisibles, 2019. Lima, Perú: INEI; 2020.
34. Basu P, Mahajan M, Patira N, Prasad S, Mogri S, Muwonge R, et al. A pilot study to evaluate home-based screening for the common non-communicable diseases by a dedicated cadre of community health workers in a rural setting in India. BMC Public Health. 2019;19(1):14. doi: 0.1186/s12889-018-6350-4.
35. World Health Organization. Global spending on Health: A world in transition. Geneva, Switzerland: WHO; 2019.
36. Sociedad de Comercio Exterior del Perú. Informe de gasto público en salud, 2019. Lima, Peru: ComexPeru; 2020.
37. Ministerio de Salud. Evaluación de los programas presupuestales de salud al I semestre 2019. Lima, Perú: MINSA; 2019.
38. Maslakpak MH, Safaie M. A Comparison between The Effectiveness of Short Message Service and Reminder Cards Regarding Medication Adherence in Patients with Hypertension: A Randomized Controlled Clinical Trial. Int J Community Based Nurs Midwifery. 2016;4(3):209-18.
39. Steinman L, Heang H, van Pelt M, Ide N, Cui H, Rao M, et al. Facilitators and Barriers to Chronic Disease Self-Management and Mobile Health Interventions for People Living With Diabetes and Hypertension in Cambodia: Qualitative Study. JMIR Mhealth Uhealth. 2020;8(4):e13536. doi: 10.2196/.
Cite as: Ruiz-Alejos A, Carrillo- Larco RM, Bernabé-Ortiz A. Prevalencia e incidencia de hipertensión arterial en Perú: revisión sistemática y metaanálisis. Rev Peru Med Exp Salud Publica.2021;38(4):521-9. doi: https://doi.org/10.17843/rpmesp.2021.384.8502.
Correspondence: Antonio Bernabé- Ortiz; antonio.bernabe@upch.pe
Received: 07/06/2021
Approved: 09/12/2021
Online: 22/12/2021